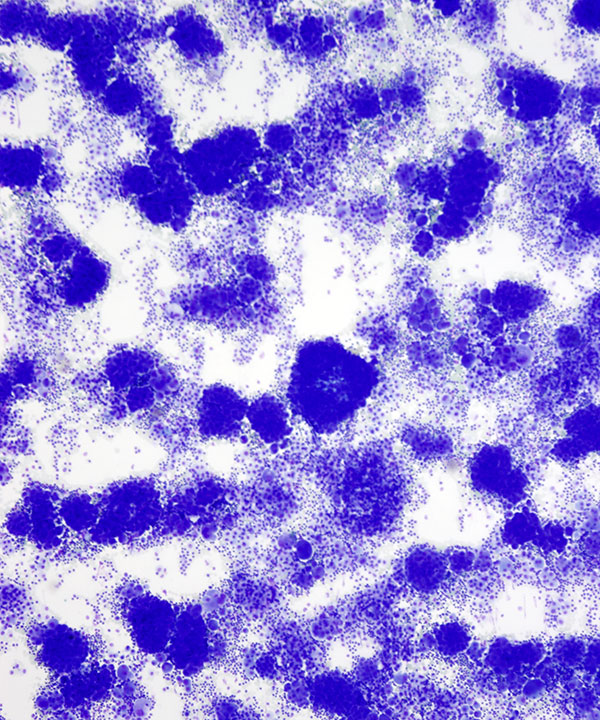
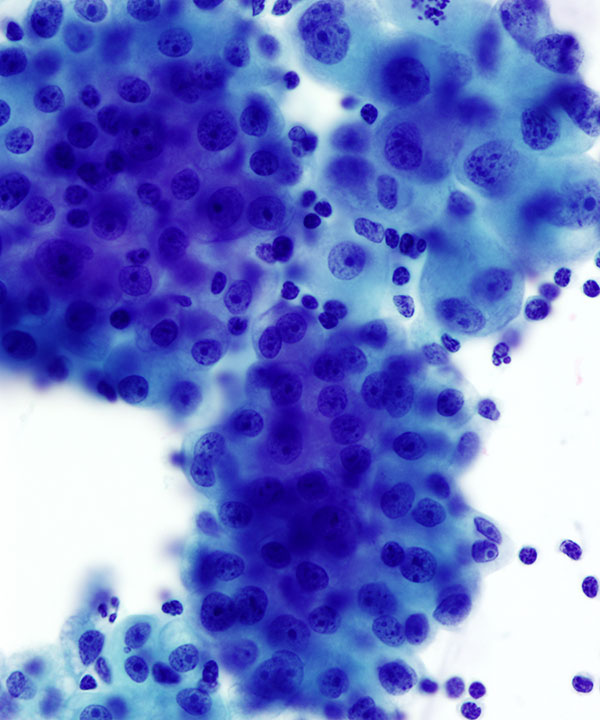
Low power: DQ stain
Highly cellular smear with large clusters of cells resembling clusters of berries
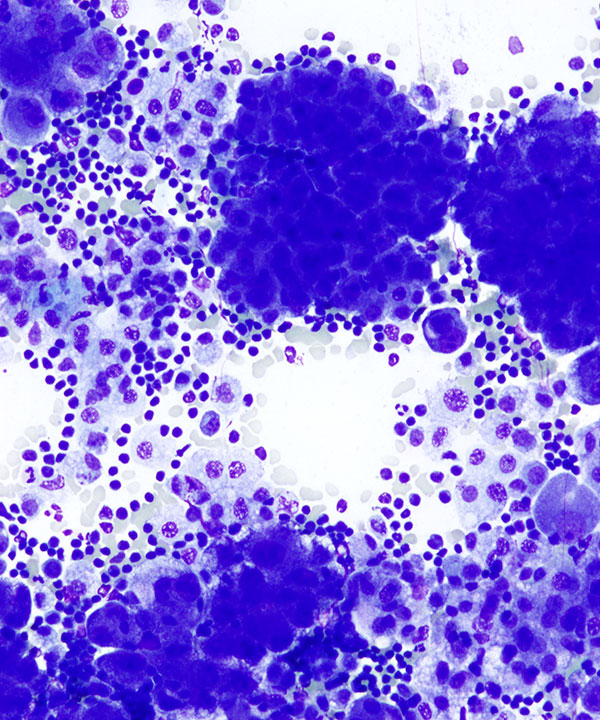
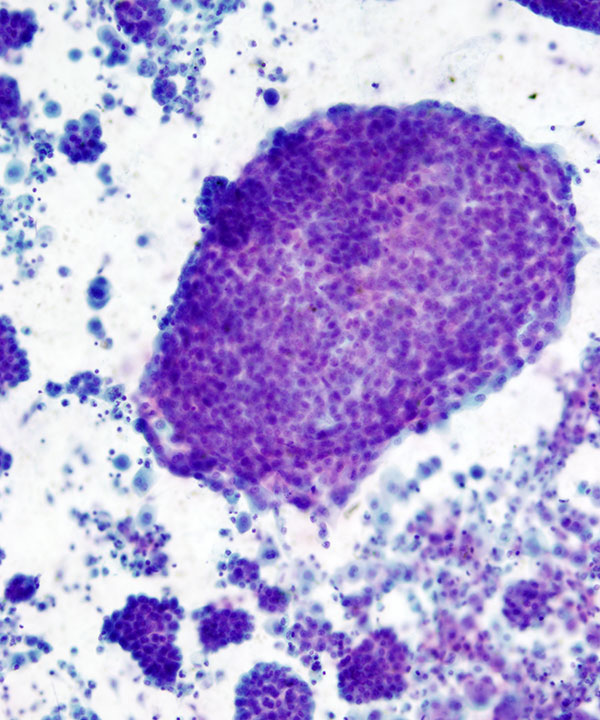
Medium power: DQ stain
Cellular smear with large clusters of mesothelial cells with rare atypia
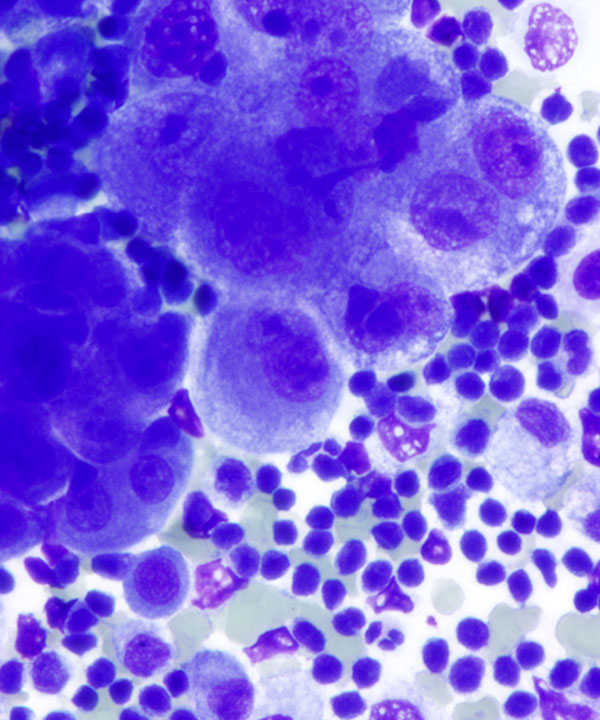
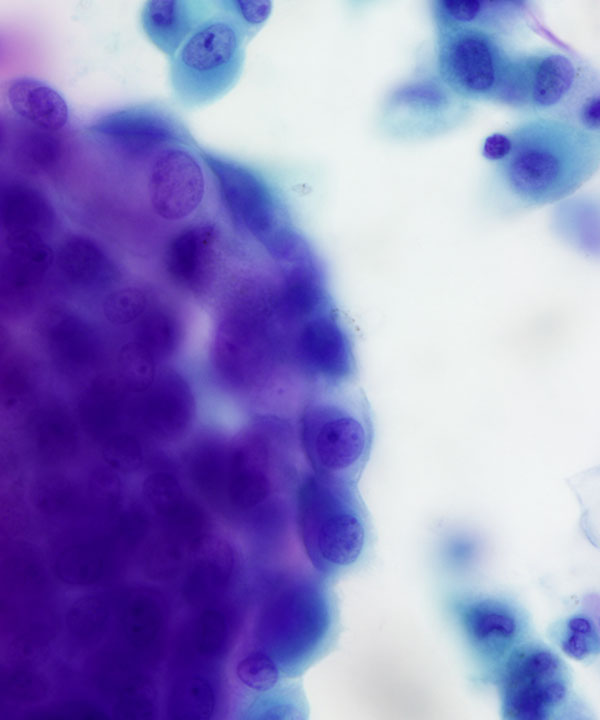
High power: DQ stain
Mesothelial cells with mild nuclear atypia, binucleation and prominent nucleoli
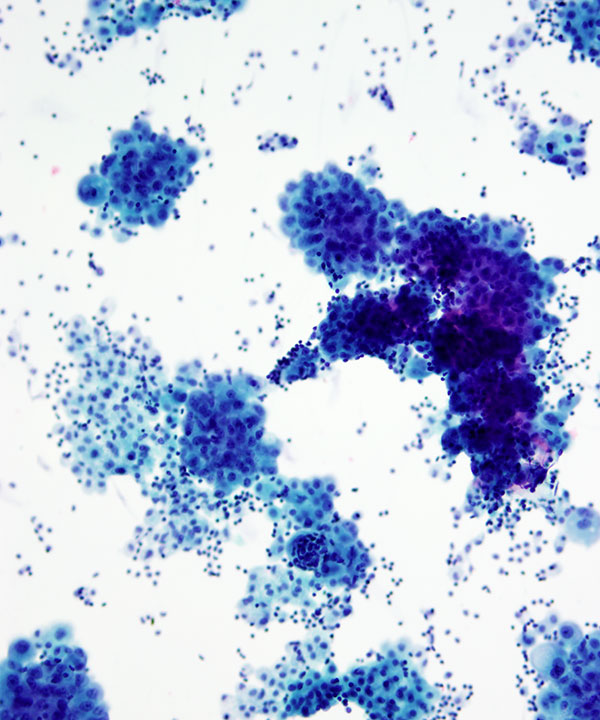
Medium power: Pap stain
Cellular smear with large clusters of mesothelial cells resembling clusters of berries with knobby contours
High power: Pap stain
Large clusters of mesothelial cells with nuclear atypia, coarse chromatin, prominent nucleoli, and dense cytoplasm
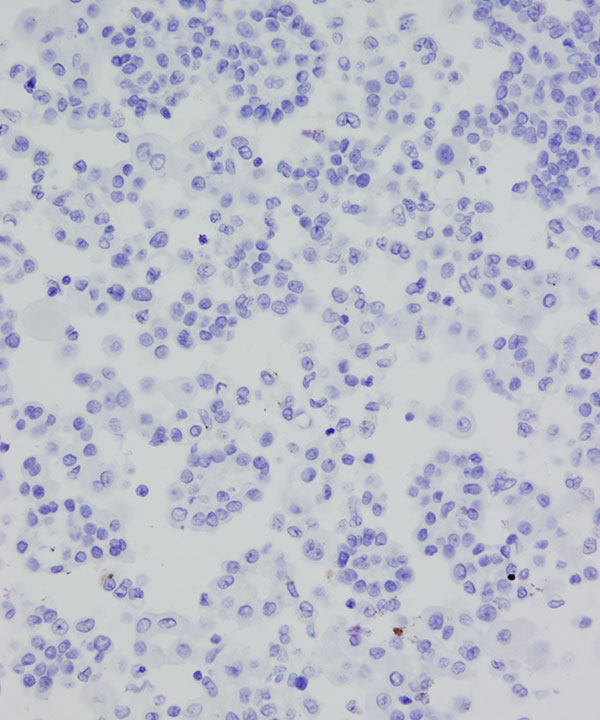
Medium power: Pap stain
Cellular large clusters of mesothelial cells highly suspicious for mesothelioma
High power: Pap stain
Knobby contour (vs cannonball-like smooth contours of adenocarcinoma)
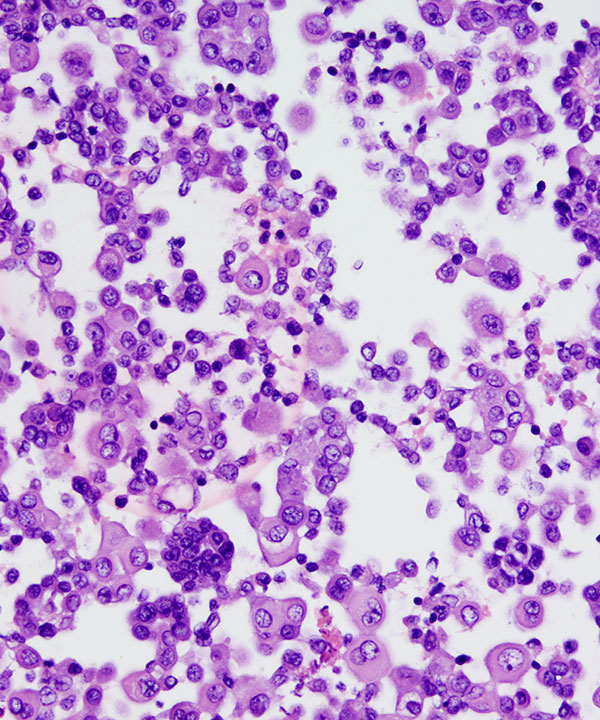
Cell block: H&E stain
Cells may be seen as clusters, small groups with a acid mucopolysaccaride core or as dispersed cells
Immunostaining is useful to delineate mesothelial origin
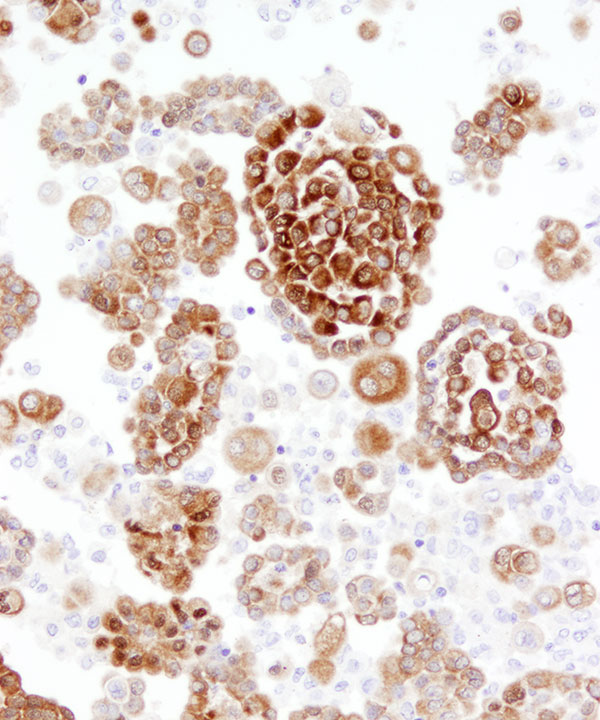
IHC for Calretinin
Typically positive in mesotheliomas with nuclear and cytoplasmic staining. Adenocarcinomas usually negative; rarely show cytoplasmic staining.
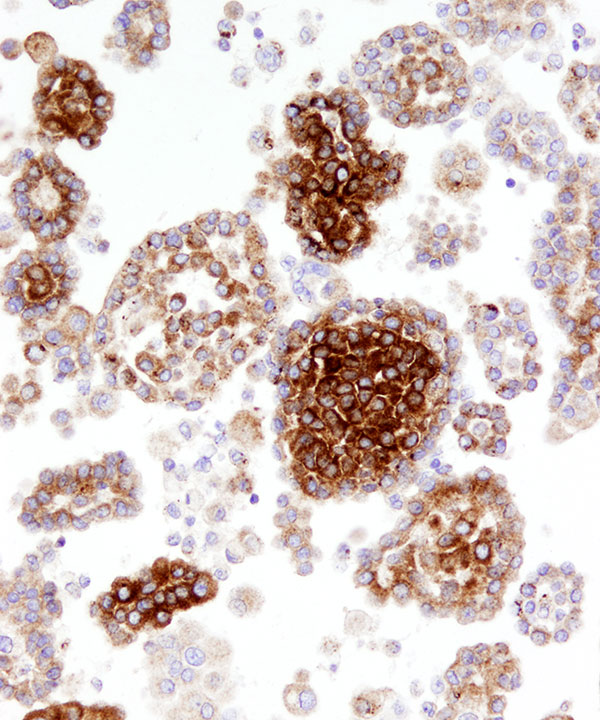
IHC for D2-40
Typically positive in mesotheliomas with membranous staining. As sensitive as calretinin and more specific than WT1. May be seen in some serous adenocarcinomas.
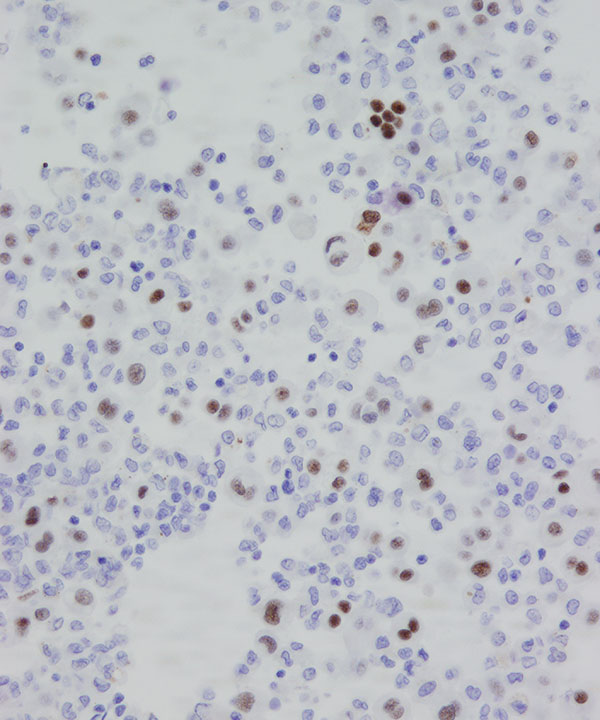
IHC for WT1
Usually positive in mesotheliomas with nuclear staining. Adenocarcinomas usually negative; except serous carcinomas.
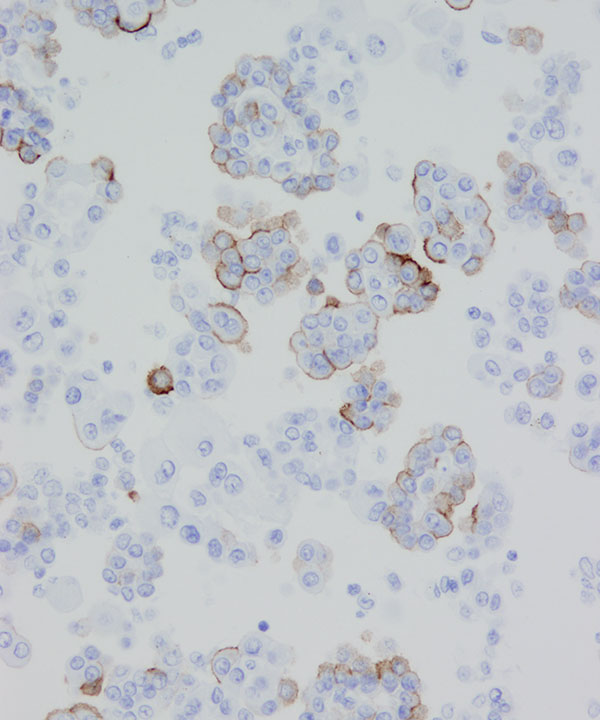
IHC for MOC-31
May be negative in mesotheliomas with exceptions as shown here. Adenocarcinomas usually positive with strong membranous staining. Shown above mesothelioma with focal staining.
IHC for MOC-31
Usually negative in mesotheliomas. Adenocarcinomas usually positive with strong membranous staining.
Features
• Mesotheliomas grow as plaques and nodules on the serosal surface of pleura or peritoneum that shed cells leading to malignant effusions.
• Cannot evaluate for invasion
• High cellularity and atypia, clues to diagnosis
• In absence of history of asbestos exposure or known mesothelioma, may diagnose as mesothelial proliferation, suspicious for mesothelioma
• Typically large clusters of mesothelial cells
• Knobby, berry-like clusters of cells
• Scalloped/knobby contours
• May have normal or high N:C ratios
• May show molding
• Cells may have windows (space between cells)
• Abundant dense cytoplasm may be present
• Cytoplasmic vacuoles may be present
• Round nuclei, may show atypia
• Often binucleated
• Nuclear membrane smooth to irregular
• Chromatin usually fine but may be coarse
• Prominent nucleoli may be present
• IHC to differentiate benign and malignant mesothelial cells are problematic. Mesothelial markers like calretinin, WT1, D2-40 are usually helpful in differentiating from adenocarcinoma cells.